TRABECULECTOMY IN CLOSED ANGLE UVEITIS GLAUCOMA A CASE REPORT Poster Presentation - Case Report - Ophthalmologist

Article Sidebar

- Trabeculectomy, Uveitic Glaucoma, Angle Closure
Abstract
Introduction : Glaucoma uveitis is caused by increased outflow resistance, which distorts the balance between water production and outflow. Trabeculectomy is better than LPI in controlling IOP in glaucoma uveitis
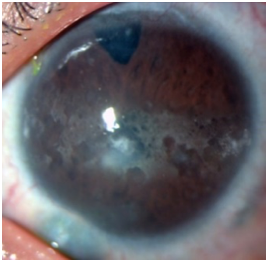
Case Illustration : Male patient aged 45 years, came to the Eye Polyclinic at Serui Hospital with complaints of very painful right eye since 2 weeks ago, the patient also complained of being unable to see at all, red eyes, headache, stiff neck, nausea and vomiting. Ophthalmological examination reveal right eye vision no light perception (NLP), palpebral edema, spasm, conjunctival hyperemia, corneal edema, shallow anterior chamber angle, iris-corneal contact, negative pupillary reflex, total pupillary block, negative fundus reflex, schiotz IOP 81 mmHg.
Discussion : The patient diagnosed as right eye acute glaucoma and treated with acetazolamide, timolol maleate eye drops, potassium aspar tablets, prednisolone acetate drops, diclofenac sodium drops in the right eye, paracetamol tablets, re-evaluate in 2 hours. The patient chose to be referred to a hospital in Surabaya. The patient came back with the same complaint and was treated the same as before, right eye surgery trabeculectomy + peripheral iridectomy with releaseable suture flap limbal base with controlled IOP results, releaseable suture sutures were removed in 2 weeks. Trabeculectomy of the uveitic eye is generally less successful because of accelerated wound healing by the postoperative fibrinous and cellular response. Antimetabolites such as 5FU and Mitomycin C are used to enhance the success of trabeculectomy in uveitis eyes (5FU, MMC). 95% success (IOP less than 21 mm Hg with 1 or no treatment) was achieved with MMC augmented trabeculectomy.
Conclusion : Increased IOP due to pupillary block causes acute glaucoma with signs of high IOP, middilated pupils, decreased pupillary reflexes, and irregular shape, corneal epithelial edema, episcleral and conjunctival vascular congestion, shallow anterior chamber, small number of flares and cells.
Full text article
References
(-)
Authors

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.